

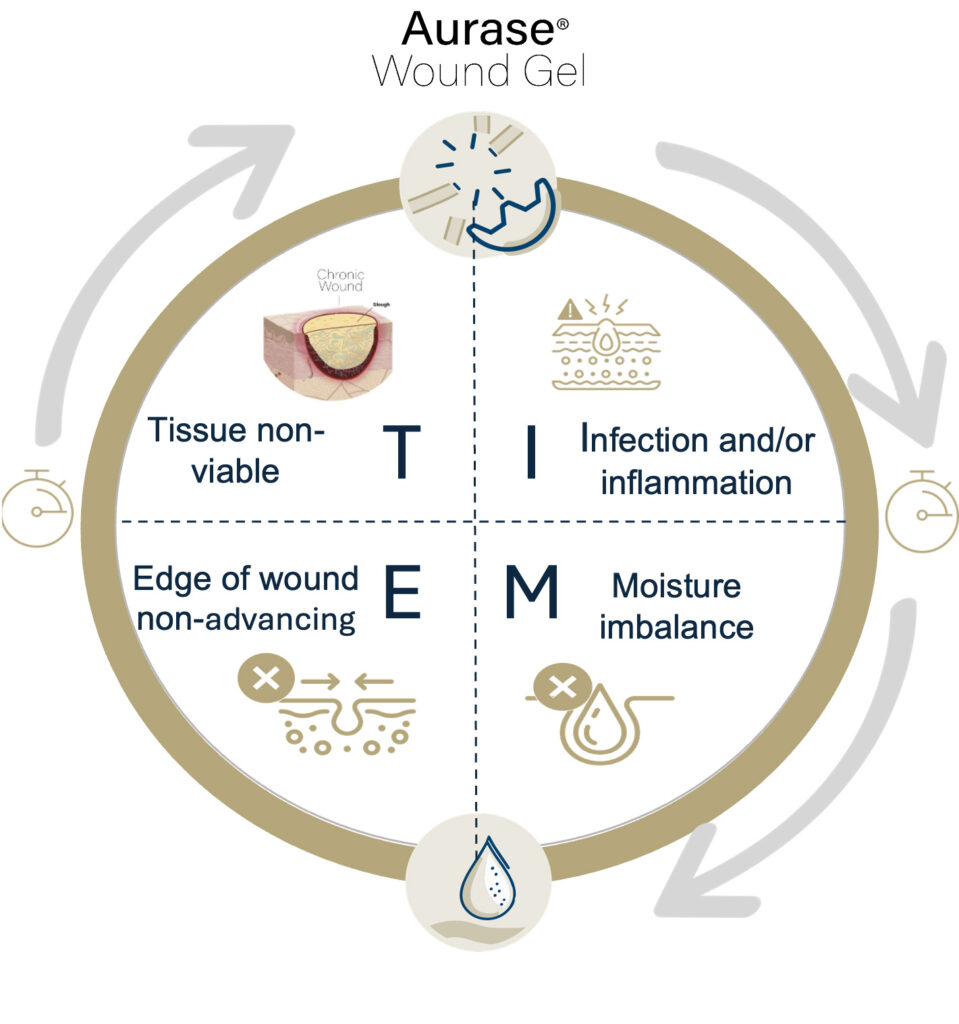
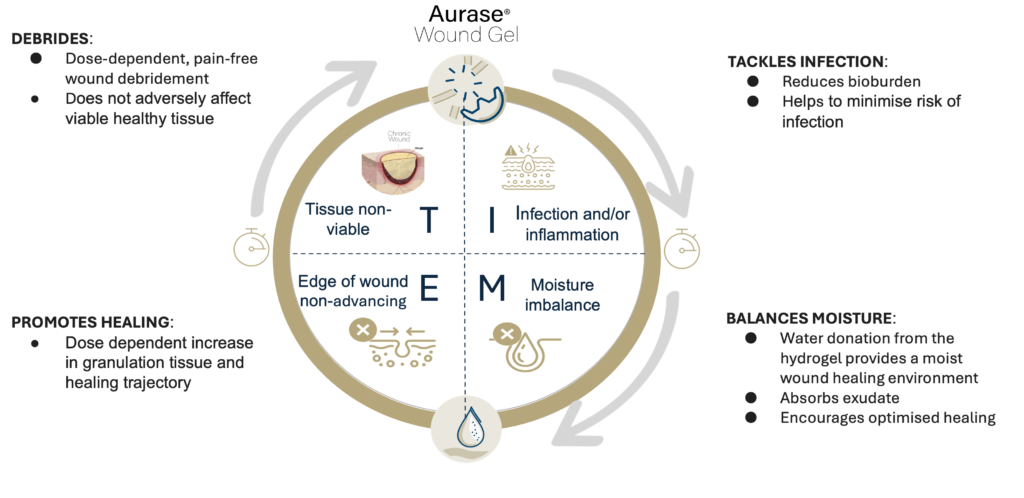
Aims to target all elements of TIME wound management paradigm
For all stages of the wound-healing journey
Pain free & not adding to patients’ pain burden
High compatibility with established wound care products

Ease-of-use in clinics & homes


Proof-of-Concept
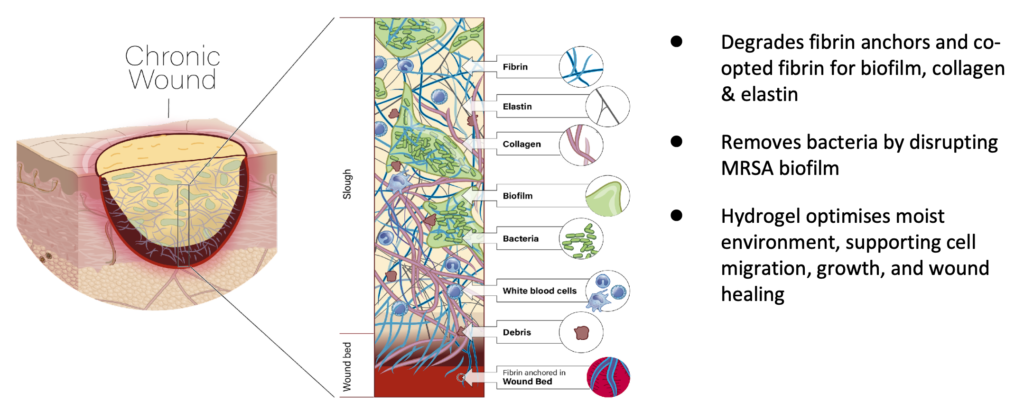
✓ Tarumase successfully debrides wounds faster
✓ More complete debridement & improved healing at increased enzyme concentrations

Strong Safety Profile
✓ No indications of systemic absorption
✓ No antibody generation
✓ No systemic effects on coagulation

Pain-free
✓ Does not add to patients’ already existing pain burden
✓ No evidence of local tolerability issues


